

TOPICS
Below is a list of topics dealing with the difficulties of treating young people with gender dysphoria. It provides the details to support why Gender Health Query is a needed organization that discusses this issue from a secular, pro-same-sex rights, non-politically affiliated perspective. We recommend reading the section “Why GHQ,” for a general understanding of the issues concerning the risks of the affirmative model in treating gender dysphoric minors, before delving into this section.
Topics analyze the risks involved in socially and medically transitioning minors, how these risks have been deemed morally acceptable based on minimal data, and how new controversial ideology about gender is affecting young people, and the culture in general. We seek to discuss these issues based on scientific data and real world observations. Topics include citations from peer-reviewed journals and quotes from gender dysphoria professionals, whenever possible. Since the demographics of young people medically transitioning, and attitudes about gender have changed so rapidly, it is necessary to provide anecdotal examples and personal observations, in some cases, for some subjects. These include the voices of homosexual, bisexual, and trans people and parents, teachers, mental health and medical providers, detransitioners, and desisters.
There is simply not enough hard scientific data around the increasing numbers of trans-identified young people and new “non-binary” identities, at this point in time, to keep all discussions based on research papers alone.
On this website we focus on risks of the affirmative model and issues around gender ideology. However, presenting information through the use of documentation, not ideology, is a priority. We acknowledge pro-affirmative model data and viewpoints, for context and balance, when necessary.
There are many sources cited in the Topics sections, and here is a complete list of references.
For a hyperlinked full outline of all subject matter please see HERE. The index may be helpful to people seeking access to quotes, examples, and scientific citations based on each specific topic or subtopic.
TERMS TO KNOW
AFFIRMATIVE MODEL: Gender identity is fully affirmed, often with medical transition offered to minors
GD: Gender Dysphoria
DESISTANCE/PERSISTENCE: Terms used for youths who outgrow wanting to be the opposite sex, versus those who maintain a trans identity
GENDER IDEOLOGY: Term used for trans/genderqueer ideology (a subset of “queer theory”), with roots in postmodernism. It states that literal biological sex is based on gender identity and that gender is a spectrum. It favors subjective experience over other ways of looking at the world.
GNC: Gender Nonconforming
FtM: Female to Male Trans Person
INFORMED CONSENT MODEL: Gatekeeping processes are removed but the patient (even a minor) is informed of medical consequences
MtF: Male to Female Trans Person
SRS: Sex Reassignment Surgery
WPATH: World Professional Association for Transgender Health
”LGBT”: This is in quotes on the GHQ website because despite its widespread use, there is no such thing as an “LGBT person” or united “LGBT agenda” and the constant use of the term creates a false impression that there is. LGB people and trans people have different needs and viewpoints between and within their populations.
1. Do children & teens with serious gender dysphoria ever outgrow gender dysphoria?
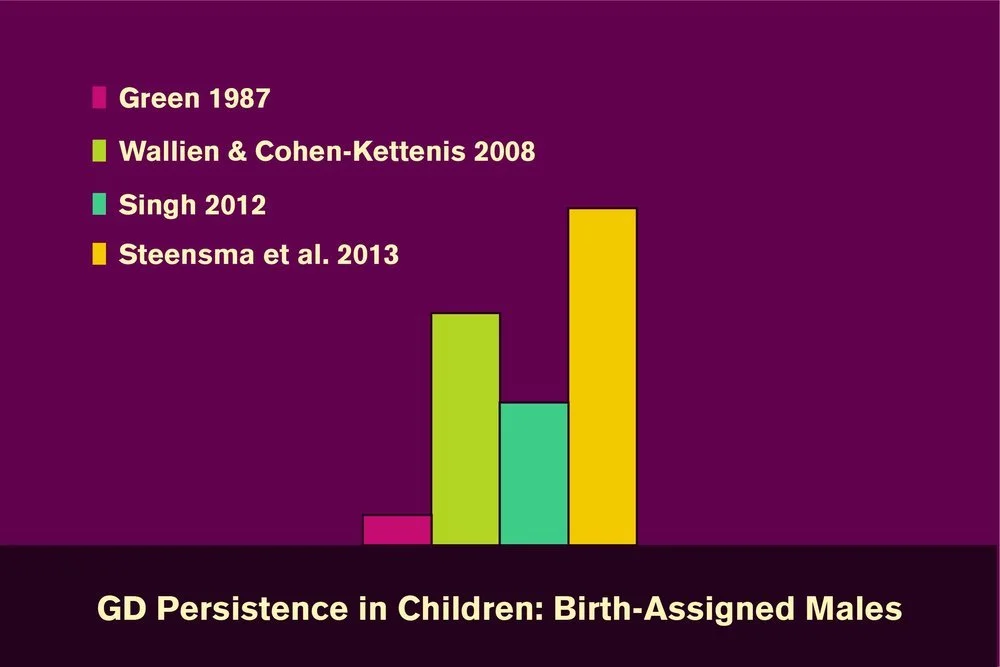
Desistance/persistence are the terms used for youth who do & do not outgrow gender dysphoria. Youth who desist are very likely to grow up gay or lesbian. Desistance data complicates the concept of childhood gender identity & use of early medical treatments on minors. Early transition is viewed as a right. Some health professionals believe a social transition may prevent desistance. Currently, some teens are also identifying as trans but then desisting.

2. Side effects & permanent consequences that result from the use of hormone blockers, cross-sex hormones, & surgery on minors
A few studies show significant improvement in the mental health of youth who undergo early transition. But there are risks & health consequences to medically transitioning as a minor, such as sterility and possible risks to bone density, cognition, sexual function, & cardiac health. There is no long-term data on this cohort, as minors have never transitioned at such early ages.

3. Are children & teens old enough to give consent?
Children are currently undergoing medical treatments starting as young as age 9, when they may decide to go on hormone blockers. Double mastectomies are being performed on females as young as 13, with large increases in females requesting this. The fact that humans do not reach brain maturity until age 25, calls into question if youth have the ability to consent to sterility & the health consequences of medical transition.
4. Affirmative model mental health professionals/doctors & statements suggesting lack of concrete knowledge of long-term safety & effects on desistance
Some psychologists & doctors have admitted to experimenting on their minor patients. Many claim that social transitions & puberty blockers are “fully reversible,” which is difficult to determine without a control group. There is often a lack of focus and discussion on youth who may outgrow dysphoria, & the likelihood they may be LGB.

5. Mental health and medical professionals have moved from a mental health screening model, to a gender dysphoria affirmative model
Some activists, as well as some doctors and therapists, view efforts to help a youth, even those with autism or mental health issues, find alternative ways to cope with GD, as transphobic. Supporting youth in coping with GD, to allow the body time to mature, is viewed as a hinderance to their identity. Several are adopting a “let the child lead” model for children & teens.
6. Examples of minors being medically transitioned without any meaningful psychological assessments
Many people are under the impression that there is a mental health screening process for minors, or that certain age restrictions are in place before they are subjected to medical treatments. This is not always the case. Even minors with serious mental health issues are being affirmed as trans, & immediately offered medical options .

7. Conversion therapy laws
These laws are being used to ensure that mental health professionals validate the trans identity of growing numbers of trans-identified minors. Some therapists think this prevents them from doing proper mental health exploration. Some say they are confused about what they can & can not say under these laws. A comparison with anti-conversion therapy laws for homosexuality is not appropriate, since that does not involve life-long consequences.

8. Regret rates and long-term mental health
Recorded regret rates post-surgery in the trans population is historically very low. Despite low regret rates, mental health problems remain high, indicating transition is not a fix-all. Regret rates anecdotally appear to be increasing, & may rise with more people now transitioning at younger ages and changing demographics towards females. Activists worry a focus on regret and detransition will lead to more gatekeeping.
9. New World Order: How will the environment gender activists created affect desistance rates & gender nonconforming young people in general?
Trans activism is changing the way children are raised, with non-binary birth certificates & parents raising “theybies.” Children are transitioned early & participate in extremely politicized transition environments. Schools are being used to reinforce concepts of gender. Medical treatments & parent legal battles are increasing.

10. Nature versus nurture: What other factors besides “innate gender identity” contribute to trans identification in young people?
There is some evidence that gender identity is innate & biologically driven. But there is also evidence that environment plays a role for some people. There is also a blurred line between trans & nonconforming LGB identities. Other factors that may influence gender dysphoria are homophobia, difficulties being a young female, parental influences, psychological issues, culture, & social contagion.
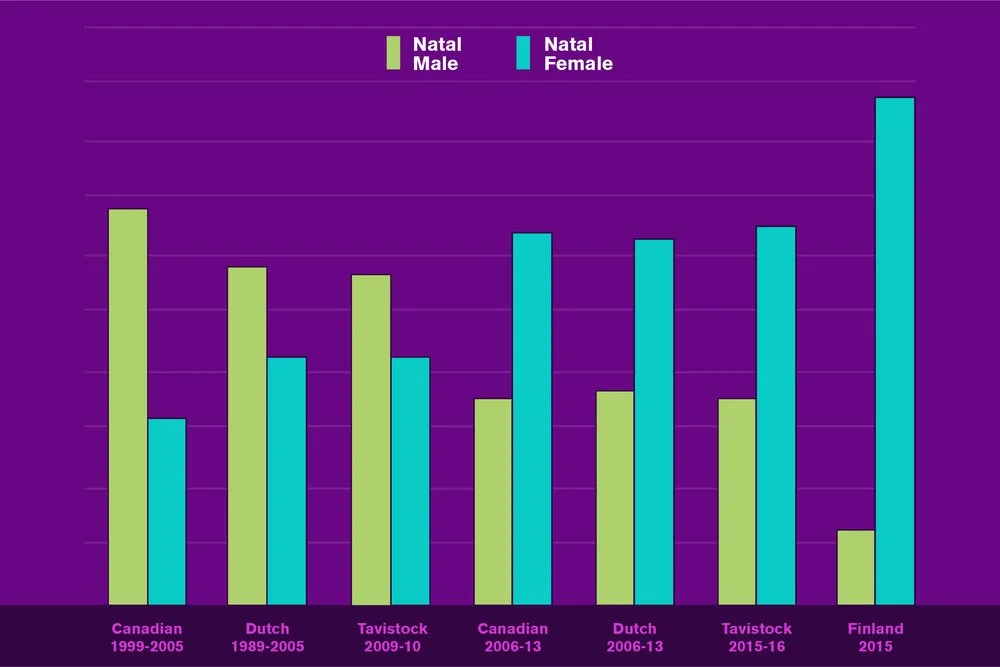
11. Why are so many females coming out as trans/non-binary?
Gender clinic data is showing very large increases of female teens & young adults. A recent study on “rapid onset GD” confirmed high numbers of females coming out as trans, with no history of childhood GD. Plastic surgeons report they are doing many more FtM/non-binary surgeries. The reasons for this may not all be increased social tolerance. They may have to do with body issues, social contagion, homophobia, trauma, & autism. Regret rates may increase in this group.

12. Cultural ripple effects, psychological consequences, & rights conflicts
Gender ideology is promoted as progressive by affirmative model advocates & “LGBT” orgs & media. Many people instead see a generation of youth who are very gender confused & sexually confused. Many feel gender ideology reinforces gender stereotypes, over focuses on pronouns, & glorifies dysphoria. There are also implications of trans activism for girls & women who are being displaced by males with GD in positions such as sports placement.

13. Gender ideology is being prioritized in educational settings when scientific validity claims are questionable, & it is controversial, even within and between people in LGB and T populations.
Postmodern “queer theory” has been accepted into schools with little analysis or concern for its effects on desistance or ability to confuse children. Gender ideology is being prioritized in educational settings when scientific validity claims are questionable & it is controversial, even among the people it purports to represent. The loudest critics of current gender ideology are gay, bi, lesbian and trans people, not “right-wing” people.

14. Problems with a politicized climate of censorship/harassment
Unfortunately a byproduct of an increase of trans visibility & activism has been hostility, threats, & attempts to censor balanced discussions around the ethics of medical treatments on minors. This is common around any discussion about childhood & teen gender dysphoria. This happens to mental health & medical professionals, journalists, educators, parents, desisters, concerned LGB people, & dissenting trans people.

15. “Transition your child without question or they will kill themselves”: Suicide risk reviewed
This is often repeated to enforce societal & parental acceptance of an affirmative model. Studies show rejecting a trans person negatively impacts mental health. However, this threat is being used by affirmative model professionals to erase concepts of mental health screening. Some are violating guidelines that suicide prevention orgs put forth to protect youth from social contagion.
16. Trans rights, affirmative model advocates, & the acceptability of false positives
Some trans people have said gatekeeping has harmed them & that they knew who they were from a young age. This creates pressure to create viewpoints & protocols that risk creating false positive medical transitions on minors. These minors are disproportionately likely to be LGB, thus potentially impacting those communities and making this more than just a trans rights issue. It involves other groups of gender nonconforming youth.

17. Moral Dilemmas: Trans Rights/Desister Rights: An objective breakdown of the pros & cons of social & medical transition of minors
People have differing opinions around the ethics of socially transitioning young children, giving tweens hormone blockers, & affirming large increases of trans-identified teens. These views can be affected by one’s own identity or status as a parent. Mental health professionals don’t all agree. There are arguments for the benefits of affirmation & there are arguments that the risks are too great.